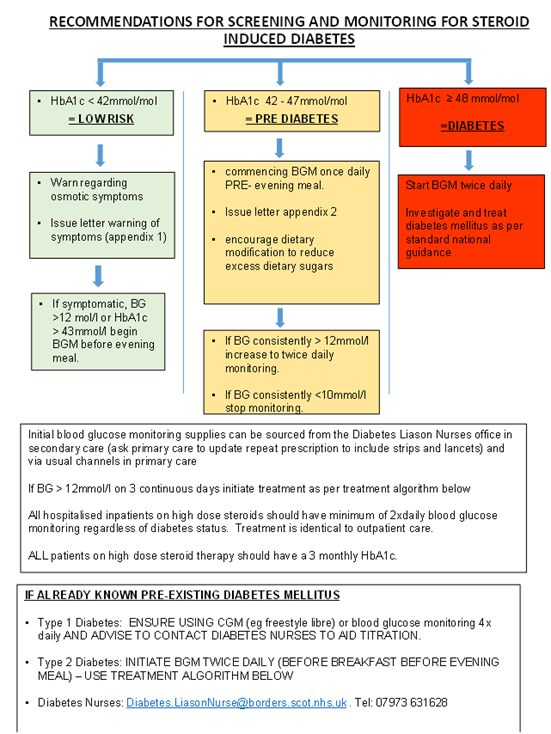
Click for full size flowchart (Recommnedations for screening and monitoring for steroid induced diabetes)

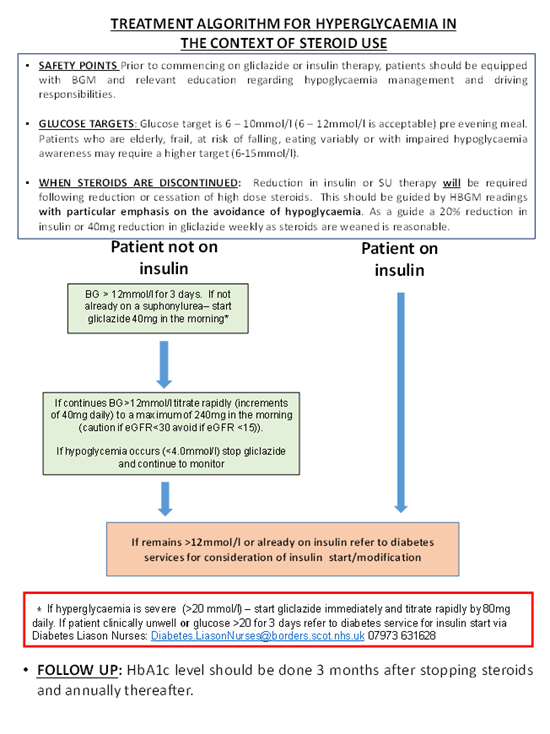
Click for fullsize treatment Algorithm (Treatment Algorithm for hyperglycaemia in the context of steroid use)
STEROID WITHDRAWAL ADVICE
- NICE Guidelines (Adrenal insufficiency: identification and management) 2024 Section 1.9 covers managing glucocorticoid withdrawal to prevent adrenal insufficiency
- Decisions to taper glucocorticoid should be made by the treating team
- Suggested tapering regimens are outlined, including a faster taper for those who have been on glucocorticoids for 4 – 12 weeks and a slower taper for those on glucocorticoids for more than 12 weeks
- Temporary symptoms including fatigue, reduction in appetite, low mood should be expected when tapering below physiological dose (e.g. 4mg).
- If signs and symptoms of adrenal insufficiency develop below physiological dose (e.g. 4 mg) on faster weaning regimen then increase to double physiological dose (e.g. 8 mg) for 1 week then reduce to 4 mg prednisolone for 1 week then wean as per slower tapering regimen
- When weaning down and withdrawing long term steroids, patients who develop symptoms or signs of adrenal insufficiency on slow weaning can be risk stratified by a morning cortisol sample (brown tube, order on Trak or by handwritten form) taken prior to steroid dose and having omitted prednisolone the previous day. This should be done once prednisolone dose reaches 4mg or less. Prednisolone should be restarted after the blood test pending results.
- Interpretation of the 9 am cortisol is as per Table below
| RISK |
MORNING CORTISOL (nmol/l)
|
ACTION |
| HIGH RISK |
<275 |
Continue 4mg prednisolone and refer to endocrinology services. (If already in secondary care, perform short synacthen test pre morning steroid does if possible)
|
| MODERATE RISK |
275-425 |
Can wean and stop prednisolone if treated medical condition allows. Sick day dosing of 10mg prednisolone (or seek medical attention if unable to take) as per steroid emergency card for 3 months.
|
| LOW RISK |
>425 |
Can stop prednisolone |
STEROID ‘SICK DAY RULES’
Patients prescribed steroids at >5mg/day prednisolone (or equivalent) for over 4 weeks are at risk of adrenal suppression and therefore may be at risk of adrenal crisis.
| Steroid |
Dose Equivalent |
| Prednisolone |
5mg per day or more |
| Methylprednisolone |
4mg per day or more |
| Hydrocortisone |
15mg per day or more |
| Dexamethasone |
500 micorgram per day or more |
Patients at risk of adrenal crisis should be issued a STEROID EMERGENCY CARD (found in patient information leaflet appendix 1 and can be found at www.endocrinology.org/adrenal-crisis or obtained from Pharmacy.
Sick day rule dosing for patients at risk of adrenal crisis is as follows (N.B. – if taking prednisolone 10mg daily or more, this is sufficient for rule 1 ‘moderate intercurrent illness’ cover and double dose not required)
Sick day rules
| Patient taking |
<10mg prednisolone (or equivalent) |
10mg prednisolone or more (or equivalent) |
| Fever, infection needing antibiotics, surgery under local anaesthetic |
Increase dose to 10mg prednisolone (or equivalent) whilst unwell or on day of procedure |
Continue usual glucocorticoid dose |
| Persistent vomiting, preparation for colonoscopy, acute trauma, surgery under anaesthetic |
100 mg Hydrocortisone IM/IV at onset/presentation/start of procedure then 50mg hydrocortisone IV QDS. Patient should be admitted for ongoing parenteral hydrocortisone if required. |
100mg Hydrocortisone IM/IV at onset/presentation/start of procedure then 50mg hydrocortisone IV QDS. Patient should be admitted for ongoing parenteral hydrocortisone if required. |
| Patients with confirmed adrenal insufficiency lasting >3 months should be seen in endocrine clinic for education about sick day rules and emergency hydrocortisone injection. |
For perioperative and obstetric management please discuss with the anaesthetic team and consult national guidance (Management of glucocorticoids during the peri-operative period for patients with adrenal insufficiency | Association of Anaesthetists – www.anaesthetists.org).
 Borders Ref Help Toolkit
Borders Ref Help Toolkit