All patients with abnormal bleeding (IMB / PCB / PMB) or excessive discharge should have a speculum examination to rule out a cervical / vaginal / vulval malignancy.
A smear is not required unless indicated by SCCRS guidance e.g. smear due or previously defaulted.
Most cervical lesions are benign and may be referred routinely to general gynaecology.
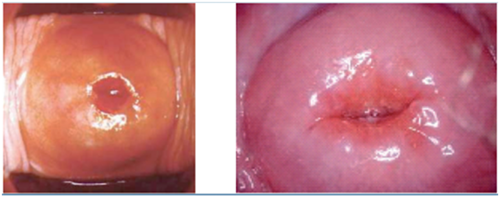

Atrophic cervix / vagina
Cervix +/- vagina may appear vascular / red after menopause due to atrophy
→ May benefit from topical estrogen if symptomatic
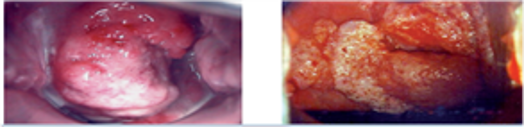
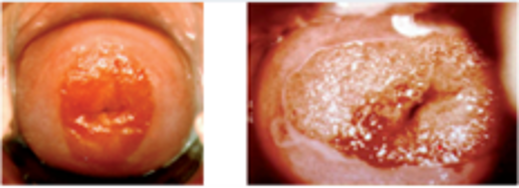
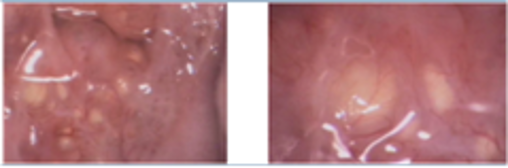
Cervical Cancer
Fungating +/- ulcerated lesions, irregular, friable
→ Refer to colposcopy as USOC
Cervical polyps
Usually benign / smooth outpouching of the lining of the cervix
→ Refer routinely to general gynaecology for removal
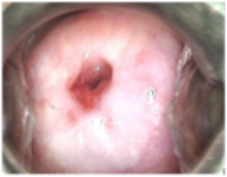
Cervical ectropion / ectopy Physiological
→ Only requires treatment if causing bothersome symptoms (PCB or excessive discharge) and patient wishes intervention
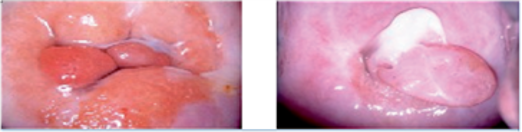
Nabothian follicles Physiological (blocked glands)
→ No intervention required
Prior LETZ treatment (at colposcopy)
Scarring / may appear like an ectropion / will persist after menopause
→ Manage like an ectropion
All the images above are with permission from the NHS Cancer Screening Programmes.
Colposcopy (USOC)
- Abnormal smears – these patients will be referred via SCCRS
- Suspicion of cervical malignancy on speculum examination
Sci Gateway -> BGH -> Gynaecology – Colposcopy (choose URGENT REFERRAL in protocol text and priority USOC)
General Gynaecology (USOC)
- Suspicion of vulval or vaginal malignancy
General Gynaecology (routine)
- Cervical Polyps – if patient is pre-menopausal the polyp is asymptomatic and the polyp is less than 1cm in diameter, there is no need to refer, and patient can be reassured
- Cervical ectropion – ONLY if causing bothersome symptoms and patient wishes intervention
Please see also http://www.cancerreferral.scot.nhs.uk/gynaecological-cancers/
Obsandgynae.mailbox@borders.scot.nhs.uk
 Borders Ref Help Toolkit
Borders Ref Help Toolkit