 Borders Ref Help Toolkit
Borders Ref Help Toolkit
Premature menopause (before age 40)
Complex medical history (VTE, MI, breast cancer etc.)
Persistent problems with side effects, lack of efficacy
Bleeding problems –see separate PMB guidance
History of hormone dependent cancer
Initial management of menopause symptoms
Premature menopause (before age 40)
Complex medical history (VTE, MI, breast cancer etc.)
Persistent problems with side effects, lack of efficacy
Bleeding problems –see separate PMB guidance
History of hormone dependent cancer
Diagnosing menopause should be based on the woman’s symptoms and age.
Healthy women >45 years with menopausal symptoms, diagnose without laboratory tests if:
The woman has vasomotor symptoms and irregular periods
Or
No period for 12 months
Or
Based on symptoms in women without a uterus.
Consider using FSH if
The woman is 40-45 years with menopausal symptoms.
Or
The woman is younger than 40years with suspected premature menopause.
Fluctuations in levels of FSH in perimenopause limit its use. FSH should not be done if taking the combined pill or high dose progestogen.
Consider HRT to manage menopause symptoms including vasomotor symptoms, psychological symptoms (including low mood that arises as a result of menopause), and altered sexual function.
The benefits of HRT are likely to outweigh the risks for women with disruptive symptoms below the age of 60 or within 10 years of the menopause.
In women with premature ovarian insufficiency (below the age of 40), systemic HRT is indicated until the age of the natural menopause (51 years) to prevent the early onset of osteoporosis and cardiovascular disease.
HRT may be appropriate for prevention of osteoporosis related fractures in women below the age of 60 years or within 10 years of the menopause if there are menopausal symptoms or other bone protection medication is contraindicated.
There is no clear evidence that SSRIs or SNRIs ease low mood in menopausal women who have not been diagnosed with depression.
The option of taking HRT is an individual decision made after a consultation with the woman which addresses quality of life, health priorities, risks (including time since menopause) benefits and personal preference.
Assessment includes:
Personal and family history of medical problems including:
Route:
Tablets are considered the first-choice formulation as they are more cost-effective and avoid problems with detachment from skin and local side-effects.
Patches may be appropriate in patients in whom there is a clinical need to avoid first pass metabolism of oestrogens (e.g. patients with liver disease, or diabetes), in those who are at risk of venous thromboembolism and those who cannot tolerate tablets or express a strong preference for patches
Avoid oral HRT if:
BMI >30
History of gallstones
VTE risks (first degree relative with provoked or unprovoked DVT. If personal history refer to secondary care)
Poor symptom control with oral HRT
Bowel disorder/ absorption problems/gastric banding
On a hepatic enzyme inducing agent
First degree relative with VTE- use transdermal HRT
Migraines- start transdermal with low dose, gradually increasing to control symptoms.
Non hysterectomised:
Perimenopausal (ie still menstruating or last period < 12 months ago)- combined cyclical
eg Elleste duet 1mg or 2mg (oral), Evorel sequi (transdermal), Femseven sequi (transdermal)
Change to continuous combined when 54 or after 5 years of use 9this reduced the risk of endomtrial cancer)
Or
Estrogen only plus Mirena
Postmenopausal (At least 12 months since last period) Continuous combined
eg Kliovance 1mg or Kliofem 2mg/ Femoston conti 1mg (oral)
Evorel conti (transdermal), Femseven conti (transdermal)
Estrogen only plus Mirena
Mirena
Note that when Mirena is used with estrogen only HRT it should be changed at least every 5 years. (Licence is for 4 years, but can be used for up to 5)
Tibolone- this is a synthetic steroid compound derived from soy. It is for women who are postmenopausal and has estrogenic, progestagenic and androgenic actions. It treats vasomotor, psychological, and libido symptoms. Risks are similar to those of continuous combined HRT but stroke risk may be higher.
It may have less effect on fibroids /endometriosis than other HRTs
Hysterectomised
Total hysterectomy, no endometriosis
Oestrogen only HRT
Eg Elleste solo 1mg, 2mg(oral); Estradot, Estraderm, Oestrogel, Sandrena gel (transdermal), Lenzetto
Hysterectomy (total or subtotal) with history of severe endometriosis- treat as if still has uterus.
Subtotal hysterectomy
As there may be a small amount of endometrial tissue within the cervix, give sequential HRT for 3 months. If no bleeding can change to estrogen only preparation.
Can also use continuous combined HRT, but breast risk may be higher.
Dose
The dose and duration should generally be the lowest effective for symptom control. Women who are newly menopausal may need higher doses than older women
Review after 3 months as symptom control and side effects can take time to settle. Thereafter review annually or sooner if concerns.
The dose of progesterone should be in proportion to the estrogen dose, please see the table below.
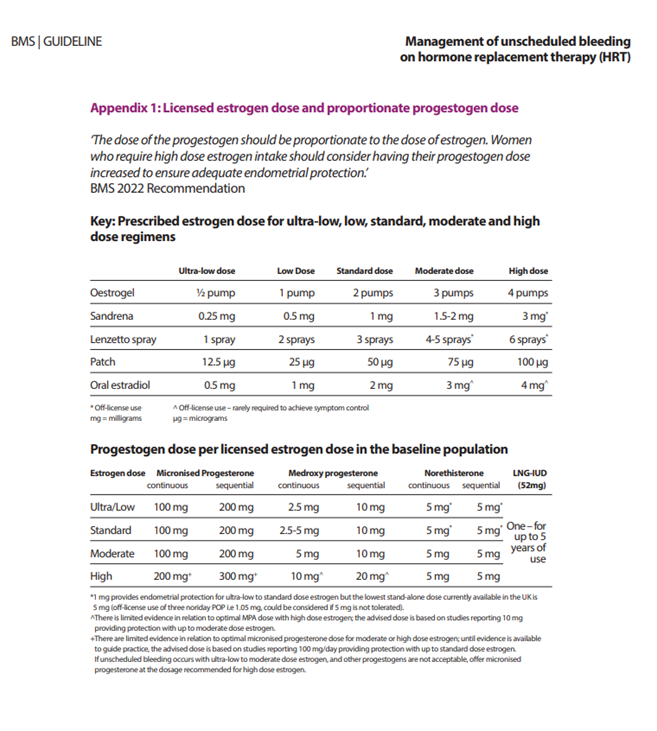
Click for full sized image
How long does HRT take to work?
Vasomotor symptoms- some improvement after 1 month, maximal by 3 months
Psychological symptoms- variable
Stopping HRT
As women get older, generally lower estrogen doses are sufficient for symptom control. The lowest effective dose should be used.
Gradually reducing the dose may limit the recurrence of symptoms in the short term but will not affect long term symptoms
Consider reducing the estrogen dose if changing a woman from cyclical to continuous combined HRT. Lower the dose to the minimum rather than extending dosing frequency.
Matrix patches can be cut so the dose can be reduced slowly.
Offer topical vaginal estrogen when discontinuing systemic HRT in women who have a history of urogenital problems or who are still sexually active.
Topical estrogens for urogenital atrophy
These can be given as pessaries, creams or a vaginal ring (Estring)
These are given initially once daily for two weeks, then twice weekly thereafter for as long as needed. No additional monitoring is required.
Vaginal estrogen is useful in treating vaginal atrophy and can also prevent recurrent UTI type symptoms in postmenopausal women
Caution is required for women with a history of breast cancer. Estriol cream or pessaries may be prescribed in women on tamoxifen after checking with the breast oncologist. These should not be prescribed in women taking aromatase inhibitors (letrozole).
Creams and pessaries may affect condom integrity.
Risks of HRT
There is an up to date risk table at the start of the HRT section in the BNF
Breast cancer
Estrogen only HRT is associated with little or no increased risk of breast cancer
Combined HRT can be associated with an increased risk of breast cancer, generally the risk is considered low. (1 in 70 extra women in their 50s with 5 years HRT use for sequential (over the next 20 year), 1 in 50 for the same group on continuous combined.
Cardiovascular disease
The risk is not increased if starting HRT before 60 years of age
The presence of CVD risk factors are not a contraindication to HRT, if optimally managed.
Diabetes
HRT is not associated with an increased risk of developing type 2 diabetes
HRT is not generally associated with an adverse effect on blood glucose in women with type 2 diabetes
A transdermal preparation should be used.
Ovarian Cancer
HRT may be associated with a small risk of ovarian cancer (1-2 extra cases /1000 women over 5 years)
Problems on HRT
Unscheduled bleeding- please see section on postmenopausal bleeding and British Menopause society guidance
Check compliance- remind patient sequential patches need to be applied in the correct order.
Management of unscheduled bleeding on hormone replacement therapy (HRT) - British Menopause Society
Lack of response
Consider the following:
Too soon for symptom response- maximal response at 3 months
Estrogen dose not high enough- consider changing to higher dose/ transdermal preparation/ Premarin 1.25mg plus supplementary progestagen.
Patient compliance problem
Symptoms not menopausal
Side effects
Estrogen and progestagen can both cause side effects.
Generally, progestagen side effects are more problematic than estrogen- note that there are different types of progestagens and women may tolerate one better than the others (see below).
There is no evidence that HRT causes weight gain, but on average women gain 10kg between the ages of 40 and 60, whether on HRT or not.
Estrogen side effects
Breast tenderness
Bloating
Leg Cramps
Nausea/Heartburn
Headaches
In general, the best approach is to wait and see- most estrogen side effects settle in 3 months.
If side effects severe, reduce dose or change route ie from oral to transdermal
Progestagen side effects
PMS type symptoms
Breast tenderness
Bloating
Headaches
Mood changes
Acne/Greasy skin
Consider changing to oral micronised progesterone (utrogestan)
Consider Mirena plus estrogen only HRT
When to refer to secondary care
Premature menopause (before age 40)
Complex medical history (VTE, MI, breast cancer etc.)
Persistent problems with side effects, lack of efficacy
Bleeding problems
History of hormone dependent cancer
Libido issues
Options are either referral to psychosexual therapy
Or
Hormonal treatment.
Consider tibolone if no cardiovascular/VTE risk factors (slightly more thrombogenic but has androgen action)
Consider testosterone supplementation.
Indication is for libido problems
Unlicensed for use in women in UK
Use in conjunction with HRT
Contraindications same as for HRT
No good evidence on long term health risks in women
Use Tostran gel 2%- 2 times per week in divided doses
Alternative is testogel 1%- I sachet in divided doses over 10 days.
Keep in fridge between doses
Check testosterone level before starting to make sure this is not higher than the normal female range
Apply to lower half of body.
Change application area regularly (or it will get hairy!)
Check testosterone levels at 3 months to ensure in normal female range. If higher than the normal range testosterone can cause irreversible coice changes, male pattern baldness and clitoromegaly
If all well yearly testosterone blood levels thereafter
National and local websites for further information
For factsheets in English and other languages on menopause, health risk and benefits of HRT, testosterone for women, hair loss, CBT in menopause and many others:
WHC factsheets and other helpful resources - Women's Health Concern
Obsandgynae.mailbox@borders.scot.nhs.uk