 GGC - Primary Care
GGC - Primary Care
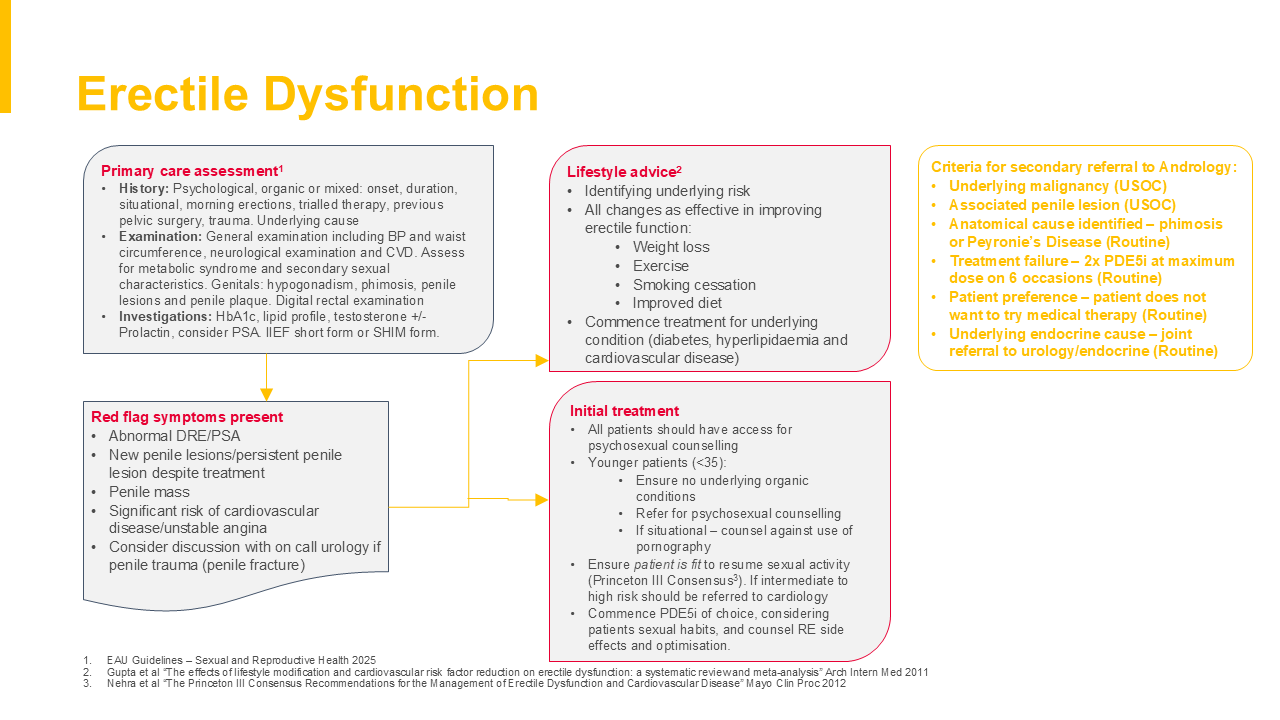
- History: Psychological, organic or mixed: onset, duration, situational, morning erections, trialled therapy, previous pelvic surgery, trauma. Underlying cause
- Examination: General examination including BP and waist circumference, neurological examination and CVD. Assess for metabolic syndrome and secondary sexual characteristics. Genitals: hypogonadism, phimosis, penile lesions and penile plaque. Digital rectal examination
- Investigations: HbA1c, lipid profile, testosterone +/- Prolactin, consider PSA. IIEF short form or SHIM form.1
Erectile Dysfunction
Warning
Click on the image to view a larger version
GGC Medicines: Drugs for genito-urinary disorders
- Identifying underlying risk
- All changes as effective in improving erectile function:
- Weight loss
- Exercise
- Smoking cessation
- Improved diet
- Commence treatment for underlying condition (diabetes, hyperlipidaemia and cardiovascular disease)2
- All patients should have access for psychosexual counselling
- Younger patients (<35):
- Ensure no underlying organic conditions
- Refer for psychosexual counselling
- If situational – counsel against use of pornography
- Ensure patient is fit to resume sexual activity (Princeton III Consensus3). If intermediate to high risk should be referred to cardiology
- Commence PDE5i of choice, considering patients sexual habits, and counsel RE side effects and optimisation. GGC Medicines: Drugs for genito-urinary disorders
- Underlying malignancy (USOC)
- Associated penile lesion (USOC)
- Anatomical cause identified – phimosis or Peyronie’s Disease (Routine)
- Treatment failure – 2x PDE5i at maximum dose on 6 occasions (Routine)
- Patient preference – patient does not want to try medical therapy (Routine)
- Underlying endocrine cause – joint referral to urology/endocrine (Routine)
- EAU Guidelines – Sexual and Reproductive Health 2025
- Gupta et al “The effects of lifestyle modification and cardiovascular risk factor reduction on erectile dysfunction: a systematic review and meta-analysis” Arch Intern Med 2011
- Nehra et al “The Princeton III Consensus Recommendations for the Management of Erectile Dysfunction and Cardiovascular Disease” Mayo Clin Proc 2012