 GGC - Primary Care
GGC - Primary Care
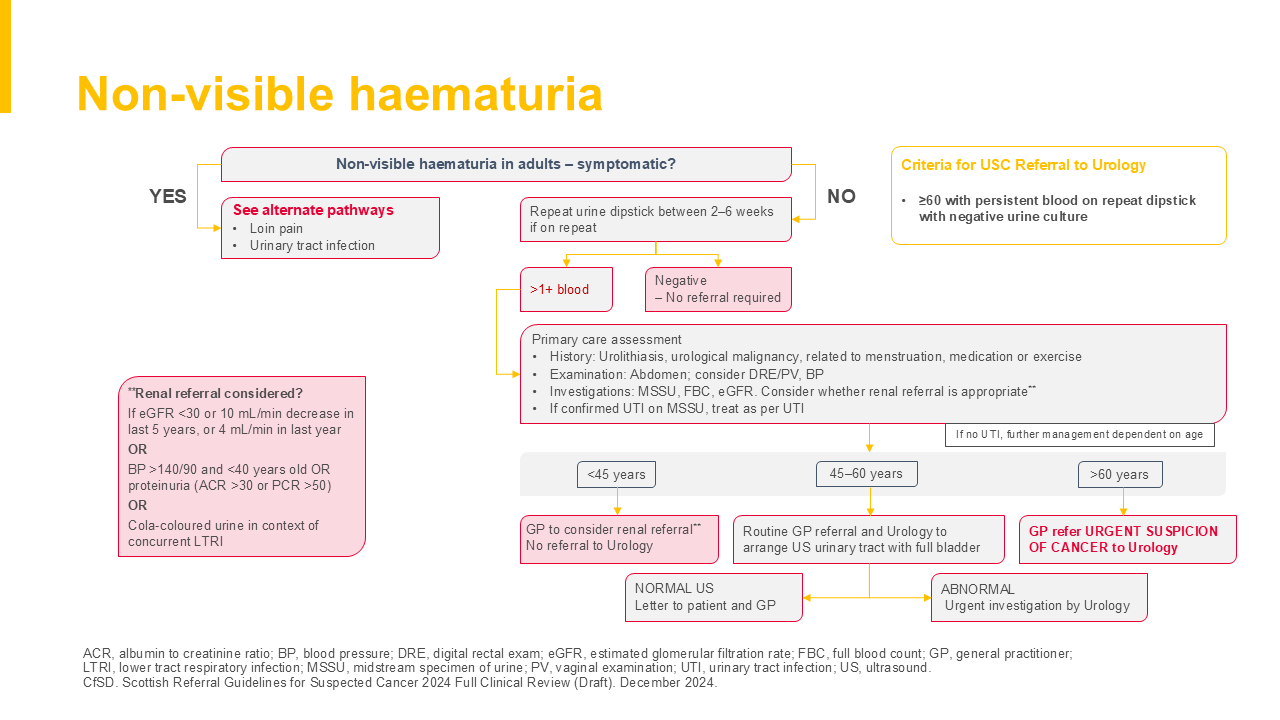
- History: Urolithiasis, urological malignancy, related to menstruation, medication or exercise
- Examination: Abdomen; consider DRE/PV, BP
- Investigations: MSSU, FBC, eGFR. Consider whether renal referral is appropriate**
- If confirmed UTI on MSSU, treat as per UTI
If no UTI, further management dependent on age
-
>60 years: GP refer URGENT SUSPICION OF CANCER to Urology
- 45–60 years: Routine GP referral and Urology to arrange US urinary tract with full bladder
- ABNORMAL Urgent investigation by Urology
-
NORMAL US Letter to patient and GP
- <45 years: GP to consider renal referral** No referral to Urology