HIV transmission elimination
HIV transmission elimination
Majority of people do not report side effects
Potential side effects
- Nausea, diarrhoea, bloating and headache can happen in about 1 in 10 people in the first months but usually resolve after four weeks
- PrEP can affect kidney function and bone density, renal monitoring is important
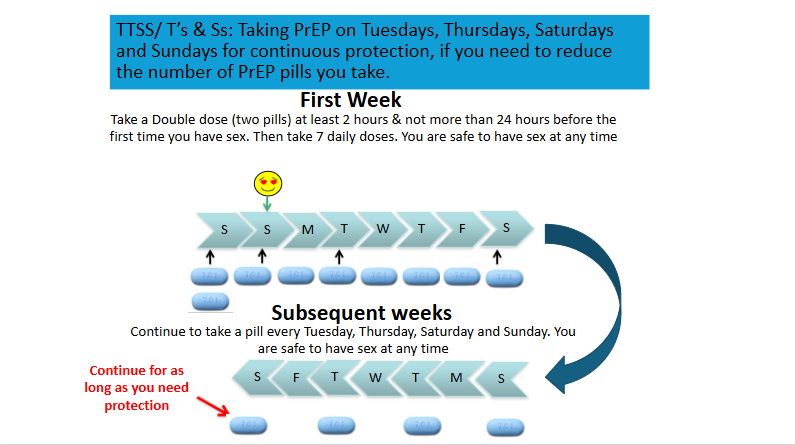
- ‘Event-based’ PrEP will help reduce the risk of renal and bone side effects as less drug exposure
Kidney function
- A small proportion of people taking PrEP have developed reduced kidney function
- Changes to kidney function reversed on stopping PrEP
- Risk is higher in older adults and/or risk factors for renal disease such as nephrotoxic drugs or family history
- Increased frequency of renal monitoring (eGFR calculated using CKD-EPI equation) to every 3 – 6 months is recommended for those with increased risk of renal toxicity.
Bone density
- PrEP may reduce bone density by 1-5%
- In studies, this was partially reversible; however, there may be a particular risk in young adults/adolescents who have not attained peak bone mass*
- Risk is also higher in those who already have low bone density related to other factors
- To date, there have been no reports of bone fractures relating to PrEP use.
*Peak bone mass is typically achieved by the mid-20s and predicts bone fractures in later life, with the period of maximal bone accrual occurring before the age of 18 years. For further information: BASHH/BHIVA guidelines on the use of HIV pre-exposure prophylaxis (PrEP) 2025