Recommendation one: A TVUS should be performed when an ovarian or adnexal mass is suspected. CT and MRI scans are not recommended for initial evaluation of pelvic cysts1.
The ultrasound request should include a detailed clinical history and examination findings including the patient’s age, menopause status, exogenous hormones (HRT, contraception or tamoxifen), and symptoms such as pain or bleeding.
A TVUS should be performed where an ovarian mass has been detected through a different imaging modality, such as CT, to accurately characterise the lesion.
Transabdominal USS should not be used in isolation but may be useful to provide supplementary information, particularly where the cyst is above the pelvic brim or very large1.
Recommendation two: Tumour markers should be assessed when a woman has been diagnosed with ovarian mass in all postmenopausal women and in all premenopausal women with anything other than simple cysts <50mm in maximum diameter.
It is recommended that ovarian masses in postmenopausal women should be assessed using CA125 only, in order to calculate Risk of Malignancy Index (RMI)3. CA125 is a non-specific test and cannot be used in isolation to determine if a cyst is malignant. A normal CA125 does not exclude ovarian cancer.
Premenopausal women with simple cysts (all B features) of <50mm maximum diameter do not require CA125 or repeat ultrasound assessment1. After discussion with the woman, it is reasonable to offer discharge to primary care.
CA125, lactate dehydrogenase (LDH), αFP and βhCG should be measured in all women under age 40 with a complex ovarian mass due to the possibility of germ cell tumours. There is currently not enough evidence to support the routine clinical use of αFP, βhCG or LDH in post-menopausal women1.
Tumour markers should be checked depending on the USS appearance, age and menopause status of the woman.
Table 1: Recommended tumour markers
| Status |
Tumour markers |
| Premenopausal, simple cyst <50mm |
None required |
| Premenopausal, simple cyst >50mm |
Ca125 |
| Premenopausal, <40y with complex cyst |
Ca125, αFP, βhCG, LDH |
| Premenopausal, >40y with complex cyst >30mm |
Ca125 |
| Postmenopausal, any cyst >10mm |
Ca125 |
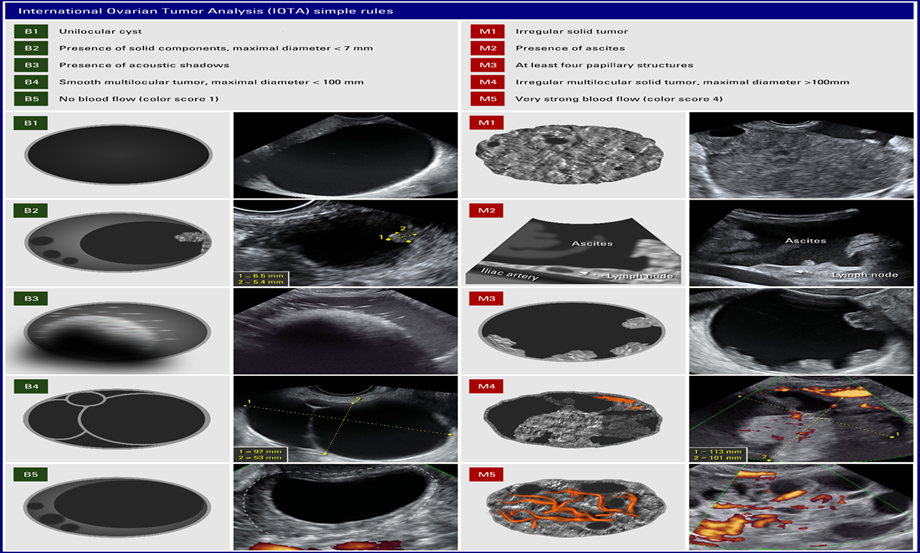
Recommendation three: IOTA Simple Rules are used to classify premenopausal women with adnexal masses. Ultrasound reporting should clearly state presence or absence of B and/or M features in its conclusion for premenopausal women. The responsible clinician should classify premenopausal patients according to IOTA simple rules into a risk group and manage appropriately.
The use of specific ultrasound morphological findings without Ca125 has been shown to have high sensitivity, specificity and likelihood ratios following the largest published study to date by the IOTA Group2. Using data derived from the IOTA Group, simple ultrasound rules were developed to classify masses as benign (B-rules) or malignant (M-rules). Using these rules the reported sensitivity was 95%, and specificity 91%.
A meta-analysis comparing pooled sensitivity and specificity has demonstrated superiority of IOTA Simple Rules (sensitivity 93%, specificity 83%) over RMI (sensitivity 44%, specificity 95%) in the evaluation of premenopausal ovarian cysts4.
Table 2: IOTA simple rules
| IOTA Group ultrasound Simple Rules to classify masses as benign (B-rules) or malignant (M-rules) |
| B-rules |
Presence |
M-rules |
Presence |
| Unilocular cyst |
|
Irregular solid tumour |
|
| Solid components <7mm |
|
Ascites |
|
| Acoustic shadowing |
|
At least 4 papillary structures |
|
| Smooth multilocular tumour <100mm |
|
Irregular multilocular tumour >100mm |
|
| No internal vascularity |
|
Increased internal vascularity |
|
| Total B score |
|
Total M score |
|
- Premenopausal women with only B features present are considered low risk for malignancy.
- Premenopausal women with any M features present and absent B features are considered increased risk for malignancy.
- Premenopausal women with any combination of M and B features are considered intermediate risk for malignancy.
Recommendation four: Postmenopausal women should be risk stratified using the Risk of Malignancy Index (RMI) by the responsible clinician into low and high risk for ovarian cancer and managed or referred appropriately. Increased risk of ovarian malignancy is suspected where RMI is ≥ 2003.
Current evidence suggests that the RMI is the most effective scoring tool to detect ovarian malignancy in women with adnexal cysts identified after the menopause, as such its use is recommended in the RCOG, NICE and SIGN guidelines on ovarian cancer.
Table 3: Calculating risk of malignancy (RMI)
|
Calculating RMI
RMI = U (0,1 or 3) x M (1 premenopausal, 3 postmenopausal) x Ca125 (u/ml)
|
| |
|
Presence |
| USS features |
Multilocular |
|
| |
Solid areas |
|
| |
Ascites |
|
| |
Bilateral |
|
| |
Metastases |
|
| U score (0 if 0, 1 if 1, 3 if 2-5 features present) |
|
- Postmenopausal women with RMI <25 = <3% risk of malignancy.
- Postmenopausal women with RMI >50 and <250 = 20% risk of malignancy.
- Postmenopausal women with RMI >200 = >75% risk of malignancy.
A systematic review of diagnostic studies concluded that RMI is the most effective scoring tool in women with suspected ovarian malignancy with pooled sensitivity and specificity of 78% and 87% respectively for a score of ≥ 200. RMI less than or greater than 200 is therefore used to discriminate between low and increased risk of malignancy respectively.
Recommendation five: Premenopausal women classified as intermediate risk for malignancy, and post-menopausal women with complex, multilocular or bilateral masses on USS where RMI <200 should be discussed with a radiologist to determine the most appropriate cross sectional imaging modality (either CT or MRI). Women <40yrs with complex cysts should have CA125, αFP, βhCG and LDH organised by the named consultant who will follow up the results.
Cases classified as benign on CT or MRI can remain under the care of a general gynaecologist, whilst those classified as likely malignant or indeterminate with suspicious features on MRI should be urgently referred to the local gynaecology-oncology team. Where CT is suspicious for metastatic disease this should be discussed urgently with the local gyn-oncology team for referral to the regional cancer MDT.
Recommendation six: Asymptomatic, low risk/benign cysts with a maximum diameter of 50-70mm in premenopausal women, and cysts <50mm with normal Ca125 in postmenopausal women, can be managed conservatively with repeat TVS and Ca125 in 3 months.
Premenopausal women
Simple cysts <50mm (all B features) in premenopausal women require no monitoring or follow up and can be discharged. These cysts are highly likely to be physiological and almost always resolve within 2–3 menstrual cycles.
For cysts 50-70mm a further TVS should be arranged after 3 months. If the cyst has resolved the woman can be discharged. If it is unchanged a repeat USS should be performed in 1 year. There is limited evidence for ongoing surveillance beyond 1 year and therefore this should be individualised following discussion with the woman, taking account of risk factors etc. If the cyst changes (increase in size, or appears non-simple) or the woman becomes symptomatic then tumour markers should be repeated and the responsible clinician should reassess risk category and manage appropriately.
Postmenopausal women
Simple cysts <10mm (U score 0) require no monitoring or follow-up and can be discharged.
If simple cyst 10-50mm (U score 0) a repeat TVS should be arranged at 4–6 monthly intervals with repeat Ca125 for a period of 1 year. If there are no changes, patients should be reassured and discharged. Further routine scans are not required unless new symptoms develop.
If the cyst changes (increase in size, or appears non-simple) or Ca125 increases the responsible clinician should reassess the risk category and manage appropriately.
Recommendation seven: Symptomatic cysts or low risk/benign cysts >70mm in premenopausal or >50mm in postmenopausal women should be offered surgical management, ideally by a minimal access approach.
Patients should be clinically assessed taking into account comorbidities, previous surgery, and fertility concerns versus the benefits of surgery. The risk of torsion, rupture and emergency surgery should be considered and discussed with the patient.
If the woman does not wish surgical management she should be followed up as per recommendation six.
Recommendation eight: Surgical management of benign ovarian masses should be performed laparoscopically unless the size of the cyst precludes this. In premenopausal women, management should aim for ovarian preservation unless oophorectomy is indicated for other clinical reasons, or is the woman’s preference. Due to the high chance of recurrence, cyst aspiration either transvaginally, transabdominally or laparoscopically is only appropriate in highly selected cases.
The laparoscopic approach for elective surgical management of ovarian masses presumed to be benign is associated with lower postoperative morbidity and shorter recovery time and is preferable to laparotomy in suitable patients. Laparoscopic management is cost effective as it is associated with earlier hospital discharge and return to work, as well as reduced febrile morbidity, less pain and lower rates of post-operative complications.
Benign ovarian cysts should be managed either by cystectomy or oophorectomy (where appropriate) as the recurrence rates following aspiration are high, ranging from 53-84% 5. Spillage of cyst contents should be avoided where possible as preoperative and intraoperative assessment can never absolutely exclude malignancy. Consideration should be given to the use of a tissue retrieval bag to avoid peritoneal spill of cystic contents.
Where possible, removal of benign ovarian masses should be via the umbilical port. This results in less postoperative pain, quicker retrieval than using lateral ports, reduced risk of post-site hernia and improved cosmesis1.
 NHS Ayrshire & Arran guidelines
NHS Ayrshire & Arran guidelines