 NHS Borders clinical guidelines
NHS Borders clinical guidelines

Infants whose mothers receive dedicated multidisciplinary pre-pregnancy counselling show significantly fewer major congenital malformations (approximating to the rate in non diabetic women) compared to infants of non-attendees. They also have fewer immediate problems and are kept in special care for shorter periods.
The Tommy’s pregnancy planning app is a useful resource for women as it covers other important health issues such as smoking and mental health, in addition to diabetes: Planning for Pregnancy | Tommy's
All women with diabetes who are planning a pregnancy should be seen at a Multidisciplinary Clinic involving an endocrinologist, obstetrician, diabetes nurse specialist, and dietician. They should be seen with their partners if possible and provided with written information.
- Full medical, obstetric and gynaecological history.
- Check thyroid function.
- Review current medications.
- STOP: ACE Inhibitors, A2 Blockers, and Statins, Review anti diabetic medication and likely stop all but metformin and insulin. Women on other agents may need replacement with insulin. Contact the local Diabetes Secondary Clinic immediately as soon as pregnancy confirmed.
- Prescribe Folic Acid 5mg daily for at least 3-months preconception and for 1st trimester (SIGN guidance).
- Screen for complications – retinal screening, U&E, urine albumin-creatinine ratio (ACR). NICE guidelines advise renal input if serum creatinine > 120 pmol/l, eGFR <45ml/min/1.73m2 or ACR > 30 mg/mmol.
- Advice on diet and weight reduction if relevant and strongly discourage smoking, alcohol and drug use and refer to cessation services if appropriate
- Educate on the importance of near normal glycaemia control.
- Instruct partners to recognise and treat hypo glycaemia with glucagon if necessary.
- Support improvements in glycaemic control including access to structured education where appropriate and consideration of optimal monitoring and insulin delivery.
Contraception
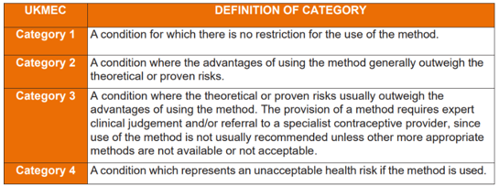
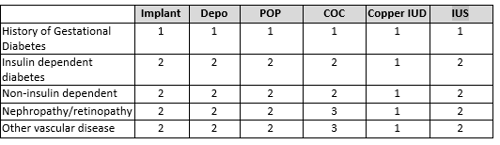
Contraception should be discussed on an individual basis with all women of childbearing age with diabetes. According to UK MEC guidance -
Optimising glycaemic control
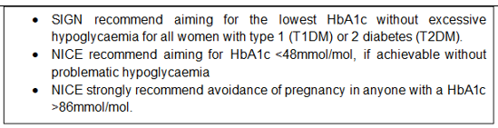
A target HbA1c of < 48 mmol/mol should be the aim, if achievable without problematic hypoglycaemia. It is, however, noted that this target may not be achievable and so failure to reach this target should not be a contraindication to pregnancy. Women should be counselled that the risks of adverse pregnancy outcomes are reduced with any reduction in HbA1c.
Women with HbA1c above 86mmol/mol should be strongly advised to avoid pregnancy.
Offer hybrid closed loop technology to all women with type 1 diabetes actively planning pregnancy. The preferred system is currently Ypsomed pump with CamAPS algorithm.
Blood glucose targets pre-pregnancy
- SIGN and Diabetes Technology Network UK guidance is to aim for sensor glucose time in range (TIR, 3.5 – 7.8 mmol/l) at least 70% of the time with < 4% below target and < 1% < 3.0 mmol/l
- Target glucose pre-meals are taken from SIGN and are extrapolated from gestational diabetes targets and suggested pre-meals/fasting < 5.5 mmol/l and 2-hour post meal 7 mmol/mol. (NICE guideline targets are < 5.3 mmol fasting, and 6.4 mmol/l 2 hours after eating)
- It is accepted that meeting these targets is very challenging
Women who are well controlled and free from complications should take 3 month’s folic acid prior to stopping contraception and keep a record of periods. Others should spend additional time optimising control and having complications investigated and treated.
Women should perform a pregnancy test if there is a lapse of 5 weeks between periods and contact their Diabetes Specialist Nurse if positive.