NHS Borders clinical guidelines
NHS Borders clinical guidelines

This document offers guidance to NHS Borders’ employees who are involved in seeking consent from a person or from a person’s proxy/welfare attorney/welfare guardian where legal posers to provide consent on the patient’s behalf in respect of assessment and treatment have been granted.
People have a legal, fundamental, ethical and moral right to decide what happens to their bodies. Healthcare staff have a responsibility to ensure they obtain valid consent from a patient before undertaking any type of care or treatment intervention, failure to do so may leave healthcare staff open to criminal charges, civil action and allegations of misconduct.
Healthcare professionals must work in partnership with their patients, respecting their right to make decisions about their care. The partnership must be based on openness, trust and good communication. Key to establishing this is respect for patient autonomy and the patient’s right to make a decision whether or not to accept any medical or clinical intervention even if refusal of such may be to their detriment. The responsibility is on the healthcare professional for ensuring that their patient is fully involved, has all the information they wish and need, understands the details and implications of the intervention including any risks that may be pertinent to them and is informed of alternative treatment options. Alternative options include the option of having no treatment. The concept of material risk introduced. Only then can the patient, and not the healthcare professional, make a decision about what they believe to be in their best interest.
There is no definitive definition of ‘supported decision making’. The Mental Welfare Commission refers to it as ‘any process in which the individual is provided with as much support and information as they need in order for them to be able to’:
- make a decision for themselves; and/or
- express their will and preferences within the context of substitute decision-making.
Any discussion about a person’s condition or treatment options should be carried out with them in a way the person can understand and, whenever possible in a place and at a time when the person is best able to understand and retain what is discussed. The discussion may be supported by the use of accurate and up to date written material, including visual or other aids.
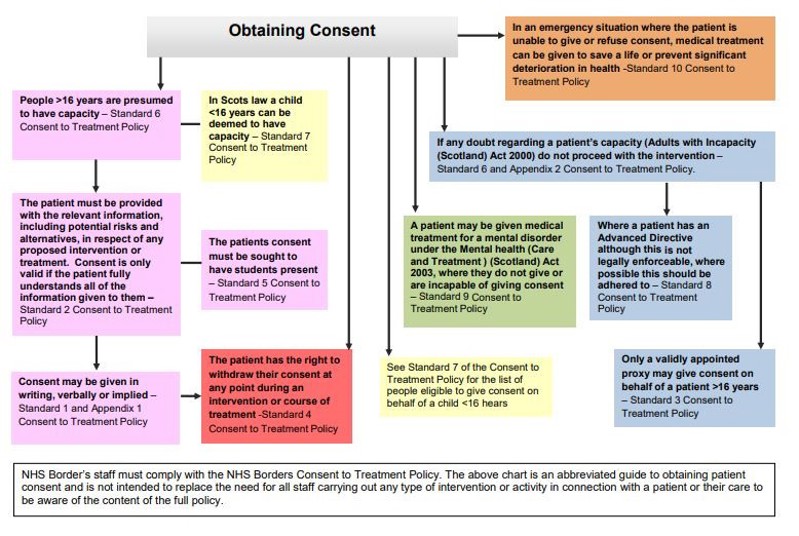
Consent:
- may be implied or explicit and may be obtained verbally or in writing
- is only valid if it is voluntary and informed and if the person consenting is deemed to have the capacity to make the decision
- is not usually a single event but is part of an ongoing process
- requires a number of steps in the process including ensuring the patient is fully informed of the risks and benefits of any proposed treatment and alternative options and the risks and benefits of no intervention
- may be withheld or withdrawn in respect of all or any aspect of the care or treatment being provided at any point during an episode of care or treatment even if given initially
NHS Borders Completion of Health Records Policy states:
It is the responsibility of all NHS Borders staff providing direct care, whether a
registered practitioner or someone in a support role, to make a note of all
encounters and interventions relating to the patient in the appropriate section of
the patient’s health record.
This includes the recording of having obtained the person’s consent, whether verbal or written, prior to a procedure or treatment being carried out and in particular where the intended procedure or treatment is of an intimate nature.
This policy relates to all patients receiving care provided by NHS Borders. The policy is applicable to all staff working in clinical environments within NHS Borders premises where care and treatment is provided to individuals. It is applicable to all NHS Borders staff who delivers care and treatment in an individual’s home and/or other community setting. Healthcare professionals must also be aware of any standards, guidance or policies pertaining to consent that have been issued by their respective professional and/or regulatory bodies.