e.g. resolving sepsis, reduction in NEWS score, improvement of infection markers e.g. WCC and CRP
CRP does not usually reflect current severity of illness or the need for IV antibiotics, and may remain elevated as the infection improves. Do not use CRP in isolation to assess whether someone is suitable for IVOST.
2: Oral route is available
Safe swallow is present, and tolerating oral route
No concerns regarding absorption
Suitable oral alternative available
For advice on drug administration via enteral tubes, consult ward pharmacist
3: Infection that DOES NOT require prolonged IV therapy
Examples of infections that usually require prolonged IV therapy include: meningitis, encephalitis, infective endocarditis, bone and joint infections, infected implants or prosthetic devices, Staphylococcus aureus bacteraemia, undrainable abscess.
For these indications, seek advice from Infectious Diseases / Medical Microbiology for antibiotic ± oral switch plan.
If all above criteria are met: suitable for IVOST
Can you STOP antibiotics? e.g. alternative diagnosis, viral infection
If not, then SWITCH TO ORAL
Are there any positive microbiology results? Select an appropriate narrow-spectrum antibiotic based on relevant culture results and individual patient characteristics (e.g. likely infection, allergy, renal function)
Are microbiology results negative (or pending)? Select an empiric oral regimen as per "Suggested empiric oral switch" table.
Most infections require ≤7 days total (IV + PO) of antibiotics.
Record the intended duration in the notes, and add a stop date to HEPMA.
If required, advice is available from Infectious Diseases, Medical Microbiology or Pharmacy.
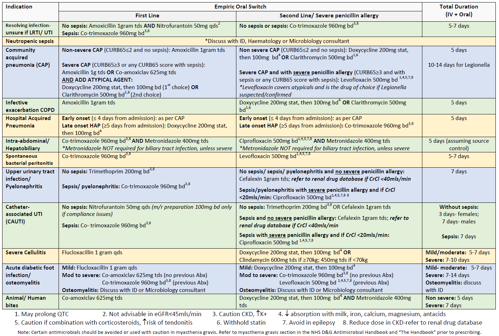
Table: Suggested empiric oral switch
If antibiotic treatment is in line with Empirical Antibiotic Guidelines and there is no positive microbiology to guide the change, then select oral regimen as per table below.
** All doses are for normal renal and hepatic function ** See BNF/ SPC/ Renal Drug Database or seek pharmacy advice regarding dose adjustments or drug interactions
Click table for larger version / pdf.
Advantages of IVOST
Potential for earlier discharge
Reduction in risk of adverse events e.g. errors in preparation are significantly higher with parenteral drugs compared with oral formulations
Reduction in risk of infusion-associated complications e.g. peripheral venous catheter phlebitis, hospital-associated Staphylococcus aureus bacteraemia, peripheral and central cannula-related thrombosis.
Saves medical and nursing time
Reduction in carbon footprint e.g. 7-day course of oral ciprofloxacin has carbon footprint of 1kg versus 67kg if given intravenous.
Reduction in treatment cost
Better patient experience
Unsuitable for IVOST? Consider OPAT.
Consider suitability of Outpatient Parenteral Antibiotic Therapy (OPAT) if patient requires ongoing IV therapy
Discuss/refer to OPAT team by contacting Ext. 33891, 33111 or 33976 or e-mail dg.opat@nhs.scot
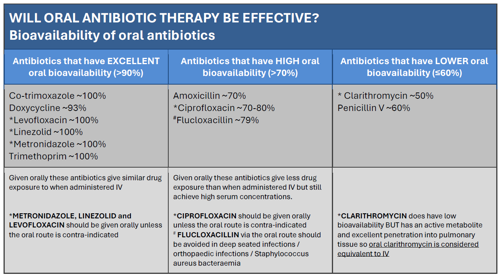
Bioavailability of oral antibiotics
Click image for larger version / pdf.
Reference: Table adapted from Hospital Antibiotic Review Programme (HARP), Scottish Antimicrobial Prescribing Group, November 2019.
Editorial Information
Last reviewed:
02/06/2025
Next review date:
02/06/2027
Author(s):
Antimicrobial Management Team.
Version:
v1.0
Approved By:
AMT (May 2025) and ADTC (May 2025)
Reviewer name(s):
Evelyn Yoong (Antimicrobial Pharmacist), AMS Team.
 NHS Dumfries & Galloway Antimicrobial Handbook
NHS Dumfries & Galloway Antimicrobial Handbook