Is there a role for PO iron?
 Preoperative assessment guidelines
Preoperative assessment guidelines

IV iron has a number of theoretical advantages over PO Iron: guaranteed dosing, effectiveness in inflammatory states with increased Hepcidin and avoidance of GI intolerance.
Disadvantages of IV iron include cost, requirement for hospital attendance, and side effects including extravasation.
Andrews et al found that 18% TKR/THR patients had Hb <120g/L. 4 weeks of PO Iron increased Hb by 11g/L in anaemic patients. Increment was greatest in microcytic patients (MCV >< 120g/L. 4 weeks of PO Iron increased Hb by 11g/L in anaemic patients. Increment was greatest in microcytic patients (MCV < 80) where Hb increased by 17 g/L7.
Petis et al found that PO Iron increased Hb by 6 g/L for THR and 7 g/L for TKR patients; ferritin also significantly increased post therapy to > 100 mcg/L8. However, THR patients received an average of 84 days of treatment and TKR patients 134 days. Use of both IV Iron and Erythropoeitin was decreased by pre-treatment with PO Iron.
In medical patients with inflammatory bowel disease, both PO and IV Iron increased haemoglobin from baseline9:
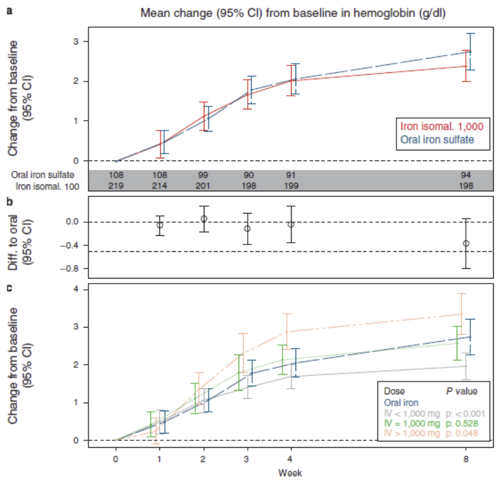
After 4 weeks of therapy, Hb increment began to slow, again suggesting that 4 weeks of therapy is required to allow response to Iron treatment.