 Vascular surgery
Vascular surgery

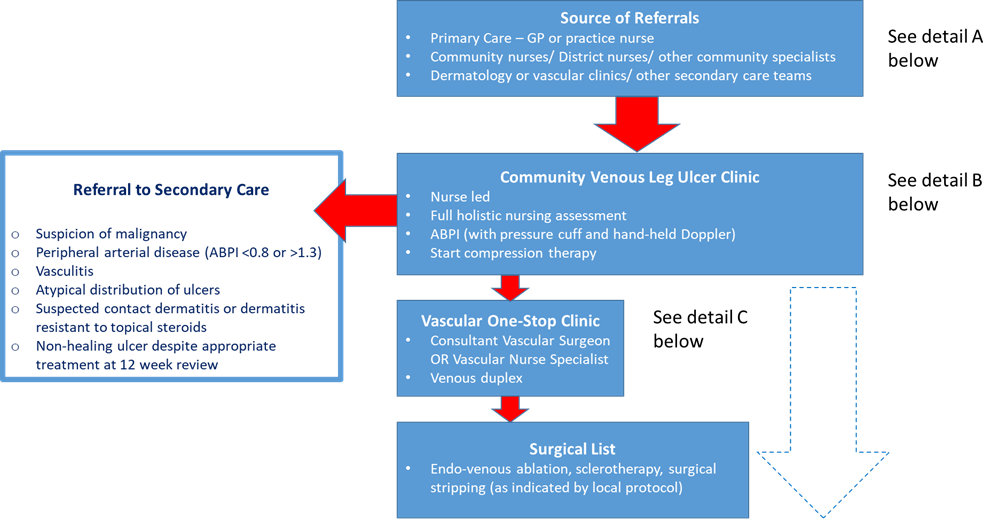
Venous leg ulcers are common and are associated with significant morbidity to the patient and cost to the NHS. Recent evidence has shown that early endovenous intervention on patients with active ulceration improves healing rates and reduces recurrence.
The National Venous Leg Ulcer Treatment Pathway should ensure timely and standardised treatment for patients with ulcers, with access to community venous leg ulcer clinics and early, streamlined referral into a vascular one-stop clinic where patients can be assessed and venous intervention planned and delivered in an appropriate timeframe.
 Scan the code to visit our website
Scan the code to visit our website