Primary survey
Use the CCABCDE approach, with heightened awareness of the nuances in older patients.
- Catastrophic haemorrhage
- Identify and control major bleeding immediately
- Older patients may be on anticoagulants or antiplatelets that can significantly worsen bleeding
- Cervical Spine
- Protect the cervical spine if the mechanism of injury suggests possible spinal involvement or there is any neck pain, altered neurology or reduced consciousness
- Hard collars can be poorly tolerated by older adults. If using, ensure proper sizing and fit, otherwise consider immobilisation in a position of comfort using a soft collar or rolled blankets, e.g. in the case of fixed flexion deformities, to reduce pain, distress and the risk of pressure damage.
- Document the need (or clearance) for C-spine precautions as soon as imaging is complete
- Airway
- Asssess for airway compromise
- Be prepared for difficult airway management in older adults with arthritis, cervical spondylosis or limited neck mobility
- Breathing
- Rib fractures are common in older adults and can be disproportionately painful, leading to hypoventilation or atelectasis, consider early regional analgesia (e.g. ESP)
- Keep an eye on possible undetected pulmonary contusions or pneumonia, especially if the patient is frail or has chronic lung disease
- Circulation
- Hypotension (SBP <110) may be significant in an older patient who is typically hypertensive; remain alert to even subtle changes in BP or heart rate
- Assess for signs of shock- older adults on beta-blockers may not mount the usual tachycardic response
- Reverse anticoagulation early if a major haemorrhage is suspected or confirmed. Use local protocols.
- Disability
- Screen for delirium using the 4AT (see here) if confusion or inattention is new or worsened.
- Check capillary blood glucose. Older adults can present with subtle hypoglycaemia or hyperglycaemia that compounds trauma severity.
- Exposure
- Fully expose the patient to identify additional injuries.
- Maintain normothermia – older adults are more susceptible to heat loss
- Look for medical alerts, medication lists or personal carer notes that can inform your assessment and management.
- Proactively seek an early collateral history to clarify baseline function and help determine overall goals of care.
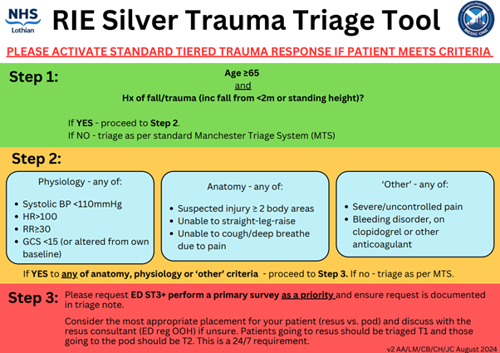
The silver trauma triage tool ensures older adults with low-energy mechanisms are flagged early. Prompt senior decision-maker input (ST3+) can help identify subtle injuries, expedite imaging (if needed) and guide next steps.
Many older adults have multiple comorbid conditions (e.g. heart failure, diabetes, renal impairment). This not only impacts resuscitation (fluid management, medication choices) but also increases vulnerability to complications such as acute kidney injury or heart failure exacerbations.
Early involvement of frailty teams, physiotherapy and occupational therapy is key, especially if extended hospital stay or rehab will be needed. A comprehensive geriatric assessment can optimise functional outcomes.
Aim to minimise ward transfers, maintain regular orientation, encourage normal sleep patterns and address sensory deficits (e.g. ensure hearing aids or glasses are in use). Pain control, infection screening and rapid screening for and treatment of constipation or urinary retention also help reduce delirium risk.
 South East Scotland Major Trauma Guidelines
South East Scotland Major Trauma Guidelines