First presentation
Most patients with symptomatic gallstones present with a self-limiting attack of RUQ / epigastric pain, frequently radiating to the back +/- nausea/vomiting.
This can usually be controlled in primary care with appropriate analgesia +/- anti-emetics without hospital admission.
Consider checking LFTs and a routine referral for USS (although may be deferred until symptoms become recurrent – please see below)
When pain cannot be managed or if the patient is otherwise unwell (septic), refer as an emergency to the on-call surgical team
Recurrent symptoms
Further episodes of biliary colic are common (50% risk per annum with 1 to 2% risk per annum of complications).
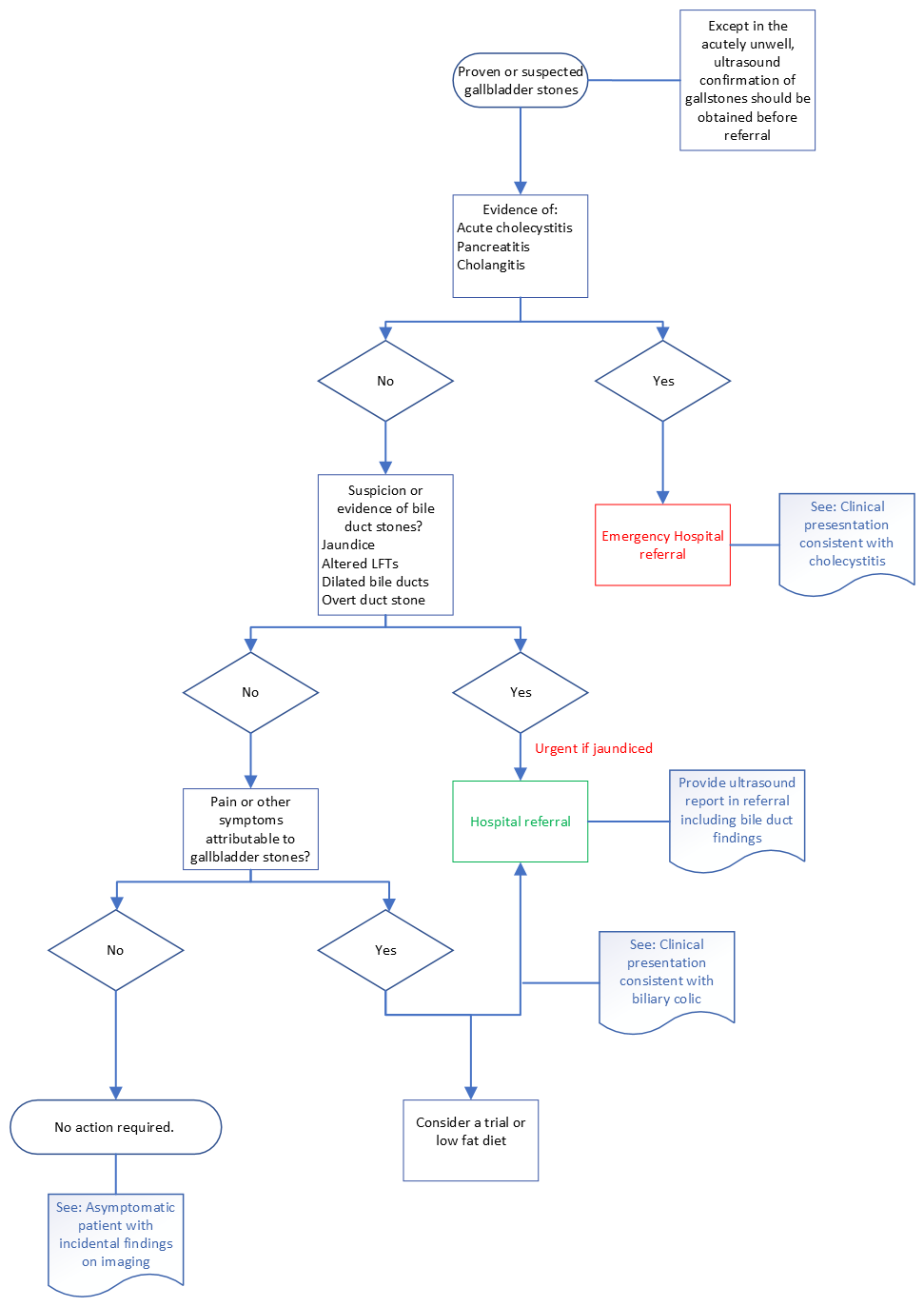
If not done following the initial presentation, arrange for LFTs to be checked and request a routine USS (unless LFTs are significantly abnormal or the patient is clinically jaundiced. (See section: Clinical suspicion of biliary obstruction)
Recurrent episodes can be prevented in around 30% of patients by adopting a low-fat diet (fat in the stomach provokes release of cholecystokinin, which precipitates gallbladder contraction).
If gallstones (including the suggestion of gallbladder sludge) are confirmed on USS, and the patient is considered fit for and would desire surgery, refer routinely for consideration of cholecystectomy
If the gallbladder is normal with no gallstones identified, consider an alternative diagnosis e.g dyspepsia.
There is NO evidence to support the use of:
- Antibiotics in the absence of signs of sepsis
- Any particular medications beyond analgesia and anti-emetics for symptom control, e.g PPIs (although biliary colic can sometimes give dyspepsia-type symptoms)
- Non-surgical treatments in the definitive management of gallstones (e.g. gallstone dissolution therapies, ursodeoxycholic acid or extracorporeal lithotripsy)
 TAM (Treatments and Medicines) NHS Highland
TAM (Treatments and Medicines) NHS Highland