When you have a spinal cord injury it can cause changes in the way your bladder works. Paralysis at any level will almost always affect bladder function.
Taking care of the bladder is especially important to anyone who has a spinal cord injury. To understand the importance of good bladder management, it is useful to understand the urinary system.
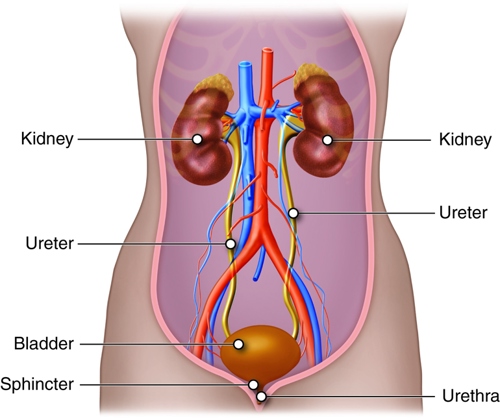
The Renal System
Kidneys: These remove waste substances from the bloodstream to form urine.
Ureters: These are two thin tubes which drain the urine from the kidneys to the bladder.
Bladder: This stores urine until it is convenient to empty.
Urethra: This is where the urine is released.
Sphincters: These are muscles at the base of the bladder, which act like automatic doors that open at the right moment to allow urine to be released.
Urination: When urine is passed from the body to the outside world at a time and place suitable to the individual.
Copyright Cenveo, licensed under Creative Commons Attribution 3.0
Why Has My Bladder Been Damaged?
Following an injury to the spinal cord, the nerve control from the brain to the bladder will no longer work. This is because the messages from the brain to the bladder are no longer being carried correctly. The brain does not know when the bladder is full and therefore cannot control emptying of the bladder.
Different Types of Bladder Function
How the bladder functions depend on where the spinal cord is damaged.
Reflex Bladder
This occurs if you have an injury at T12 or above. The nerves that cause your bladder to empty are still working. When the bladder is full, a reflex will automatically trigger it to empty, although you may have no control over this.
Flaccid Bladder
This occurs if you have an injury below T12. The reflexes are absent or weak, therefore the bladder will continue to fill, when the bladder overfills, dribbling occurs.
Mixed Bladder
This can occur when there has been only partial damage to the spinal nerves. Results can be very mixed. You may have the feeling you need to go the toilet but have no control over it, or you may have no feeling but may be able to pass urine. Management will depend on your symptoms.
Urodynamics
Urodynamics is a diagnostic test to assess the function of the bladder. This is achieved by inserting special catheters into the bladder and rectum and filling the bladder with sterile fluid to measure bladder pressures.
The information gained from this test can help your spinal doctor plan how to manage your bladder symptoms. This procedure is carried out to determine the best method of bladder management and if specific medication is indicated.
Methods Used for Managing Your Bladder
The methods to manage your bladder will depend on:
Your type of injury
What is suitable for you
Your nurses, doctors and key workers will help you through this process by offering advice, guidance, and support both as an inpatient and outpatient.
Bladder training
Bladder training is a process to teach you how to manage and empty your bladder. The type of bladder training depends on how your bladder behaves.
Catheters
As part of your bladder management, you may have a catheter. There are different types of catheters. After your injury we insert an indwelling catheter as this gives health care staff information about your kidney function.
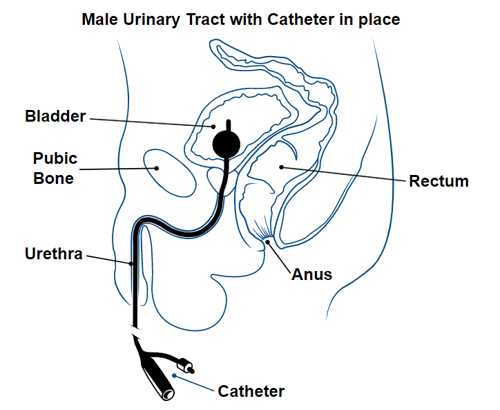
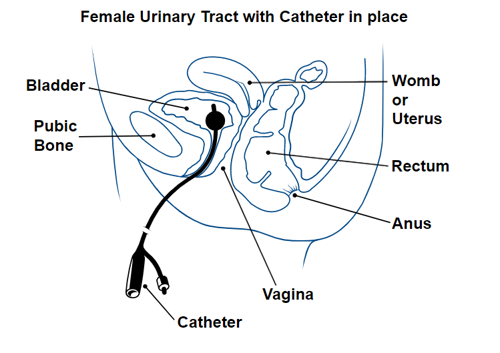
Indwelling Catheter
This catheter is inserted into the bladder through the urethra. Once inserted, a small balloon is inflated with water to keep it in place. A catheter bag is attached to the catheter which can be worn on the thigh or calf. We recommend an indwelling catheter is changed every 6 weeks to reduce the build-up of sediment and prevent blockages.
Staff will show you how to insert an indwelling catheter. If you have the hand function you will be supported in changing this yourself, which is a vital skill to have in an emergency. If you do not have the hand function, you can direct someone else to do it for you.
Suprapubic Catheter
The doctor will make a small cut above the pubic bone and then insert the catheter directly into the bladder through the abdominal wall. A drainage bag will be attached to the catheter which is then attached to the thigh or calf. We recommend this catheter is changed every 6 weeks.
The first catheter change is carried out by a doctor, however if the change proves straightforward then a suitably trained nurse can carry out any subsequent changes. The aim is to increase the diameter of the catheter tube as this helps to maintain the suprapubic site and allows for urine to drain more easily and quickly.
The new catheter should be inserted as soon as the old one is removed, to prevent the cystostomy (opening) from closing over. Timing of suprapubic catheter changes can vary, however whilst in hospital we aim to change them every 6 weeks. This is often extended in the community setting.
Indwelling Urethral Catheter and Suprapubic catheter prior to inflation
Indwelling Urethral Catheter and Suprapubic catheter after inflation
Intermittent Catheterisation (ISC)
Intermittent catheterisation allows you to empty your bladder regularly without having to wear any appliances such as a catheter bag. You insert a catheter directly into the bladder through the urethra every 4 hours. You empty the bladder then remove the catheter. Before you start using intermittent catheterisation, your nurse will discuss this with you and will teach you how to do this.
Please note, it can take several days for you to learn how to do this. There is equipment available which can make it easier for you to insert the catheter. When using intermittent catheterisation, we recommend that you drink 2 litres of fluid each day.
If you have a reflex bladder, we can use medication to dampen that reflex down so you remain continent until you do your intermittent catheter. If you are doing ISC you will also be shown how to insert an indwelling urinary catheter as there will be times when this method is more appropriate (for example going on a long journey or when you are going to be drinking more fluids).
Female Speedicath ISC
Male Speedicath ISC
Lo Fric ISC
Coloplast Luja ISC
Sheath Drainage
Men with a reflex bladder may use this form of bladder management. A sheath is a self-adhesive sheath or condom which will be measured for you. This is applied to the penis and attached to a leg bag which is then attached to your calf or thigh. You should replace the sheath every day to prevent infection and check your skin. We encourage the natural reflex to work by tapping the lower abdomen - the aim is for the bladder to contract and urine to be expelled.
To ensure the bladder is fully emptied, the nursing staff will carry out a post-voiding bladder scan. If the bladder is not fully empty (i.e. has more than 100mls present) then an intermittent catheter will be placed by the nursing staff. This will help to prevent the risk of infection. The reflex can take some time to re-establish itself and medication can be used to help stimulate the reflex.
Due to the female anatomy, there is no provision for reflex emptying because there are currently no suitable means of collecting the urine without causing lasting damage to the skin.
Sheath prior to use
Rolled out sheath
Problems that can arise with catheters
Common Problems
Signs and Symptoms
Treatment
Urinary Tract Infection (UTI)
This occurs when there is a build-up of bacteria which will divide rapidly and attack the lining of the bladder and cause infection.
Cloudy Urine
Drink plenty of fluids.
Remember in hot weather that you will need to drink more. You will also have to drink more if you have loose stools or if you have an infection. This is because you will need to replace the fluids lost from sweating and loose stools.
Increased sediment
Take a urine sample to your GP to determine if an infection is present.
Strong odour from urine
Everyone's urine has an odour, but if the odour is stronger than your normal then you should drink more fluids and contact your GP as you may need antibiotics.
Raised temperature
Flu-like symptoms
Increased spasms
Incontinence
Leakage of urine
You almost certainly have a UTI. You should increase your fluid intake and contact your GP for antibiotics.
You should state clearly that you have a spinal cord injury and the symptoms of a UTI and that you require antibiotics. It is also recommended that you change your catheter.
To treat your flu-like symptoms, you can take paracetamol. This will help bring your temperature down.
Be mindful that your skin may mark more easily so please check your skin and reduce turn times if required.
If you frequently experience UTIs then you can consider taking vitamin C 1000mg daily and changing the type of catheter you are using.
If symptoms persist, then please consult your GP for preventative treatment or your Spinal Liaison Nurse.
Dysreflexia
If your level of injury is T6 or above, then a severe UTI may trigger dysreflexia.
This is more likely if you are using intermittent catheters. If you using these catheters, then it would be advisable to use an indwelling catheter until the UTI resolved.
Having an indwelling urinary catheter will allow you to increase your fluid intake.
Blocked Catheters
This is when the catheter is blocked (often with sediment or calculi) preventing urine from passing.
No urine or old cold urine in the catheter bag.
Distended or swollen abdomen.
Increased spasms.
By-passing or leakage of urine.
Autonomic dysreflexia.
If in doubt, then remove the catheter and re-catheterise, making sure urine is draining before inflating the balloon.
Find out what has caused the blockage. Increase your fluid intake to prevent sediment and calculi building up.
If your catheter is blocking frequently contact your GP and or Spinal Liaison Nurse for advice.
Bladder or Kidney Stones
These are tiny granules that can grow in size and block the catheter tube. You are more prone to these following a spinal injury because you are less mobile, and due to the loss of calcium from your bones.
Difficulty passing urine
Visible sediment in the bottom of your urine bag or catheter tube
Frequently blocked catheters
Blood in your urine
Frequent UTI
Increased spasms
Autonomic dysreflexia
Always make sure the catheter is draining and regularly check your leg bag.
Increase your fluid intake.
Reduce foods high in calcium e.g. cheese and milk.
Keep your urine slightly acidic. This allows the chemicals to remain dispersed in the urine and not form stones.
Cranberry juice (if you are not on warfarin), vitamin C and citrus fruits can help keep urine acidic.
Every year have a kidney, ureters and bladder x-ray and renal ultrasound to check for kidney or bladder calculi (stones from sediment).
Supplies and Contacts
When you are in hospital, nurses will try different catheters according to your needs and help you choose what works best for you. Before you go home, the staff will discuss what supplies you will need.
They will liaise with the continence suppliers and discuss the most suitable way for you to get these supplies.
All this information will be on your discharge letter, which we will send to your GP and district nurse. If there are any problems with supplies when you go home, please contact your district nurse for support and advice.
Our liaison service will also offer you support and advice and liaise with your district nurses.
 The Queen Elizabeth National Spinal Injuries Unit
The Queen Elizabeth National Spinal Injuries Unit