***Example – for adaptation in NHS Boards***

Trial without catheter (TWOC)
Patient information leaflet
This leaflet provides information for patients with a urinary catheter who are expecting their catheters to be removed, either in the urology clinic or in the community. It aims to answer the most common questions and manage patient expectations regarding the TWOC.
Note: This leaflet is tailored to NHS Highland due to its unique geography and long distances some patients may need to travel to their nearest hospital.
What is TWOC?
It is the procedure of removing a urinary catheter. Catheters can be either urethral (catheters in the urine pipe) or suprapubic (catheter through the abdomen). Catheter removal must take place in a safe environment allowing the patient to manage outcomes of catheter removal. Following removal, it must be confirmed that a patient is able to pass urine spontaneously.
Where can TWOC happen?
TWOC can be booked either in a hospital setting, for example, the Highland Urology Centre in Raigmore Hospital, the outpatient department in the rural General Hospitals, or in the community carried out by community nurses, either in GP practices or by home visit.
How to prepare for TWOC?
Before your appointment, make sure to drink plenty of non-alcoholic fluids. If there are any symptoms of urinary infection or bleeding, please inform the nurse before your appointment.
What does the TWOC involve?
When you attend the appointment the nurse will explain the process, verbally consent you to remove the catheter and explain the TWOC process fully.
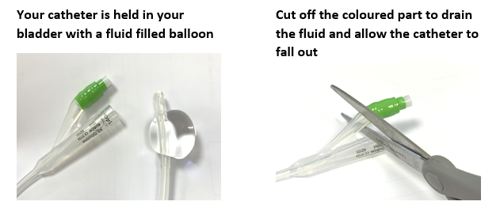
The catheter stays in place by inflating a balloon, filled with water, inside the bladder. During the TWOC the nurse will deflate the balloon using an empty syringe and gently withdraw the catheter out of the urine pipe.
If the TWOC is arranged in a hospital setting, you will be asked to drink plenty of fluids and to pass urine twice. After each void your bladder will be scanned to make sure you are emptying your bladder satisfactorily.
If the TWOC is arranged in the community setting, the nurse will advise you to drink plenty of fluids and empty your bladder in the toilet. You will receive a follow-up phone call in the next few hours to check that you are emptying your bladder satisfactorily. If you are unable to pass urine the community nurse will advise you about the next step.
If you do not pass urine within 4 hours after the removal of the catheter; you are passing only small amounts of urine; you have abdominal pain; or have not yet received a phone call from your community nursing team, you should contact them as soon as possible.
How would the TWOC be deemed successful?
Either by confirmation of satisfactory bladder emptying on bladder scanner (hospital setting) or subjectively by receiving patient feedback on voiding (in community setting).
What to look out for after a successful TWOC?
You should drink plenty of fluids and empty your bladder regularly. You should also get in touch with your nurse, GP or out of hours service if you have any signs of infection or urine retention, for example;
- Difficulty or inability to pass urine
- Lower abdominal or back pain
- Blood in the urine
- High temperature
- Cloudy or smelly urine
How to contact urology department?
Tel:
Email:
For more information regarding TWOC please visit the British Association of Urological Surgeons (BAUS) website: www.baus.org.uk
Or simply scan the QR code provided to take you to the website;

[Clinician name and job role]
August 2025
 Urology pathways
Urology pathways